Your dictation app is wrong about “metformin” a non-trivial share of the time. Your malpractice carrier knows. The plaintiff's attorney who will eventually pull the chart from a billing dispute knows. And the generalist AI vendor selling your practice on “we transcribe everything” is hoping you do not notice. Until this week, the answer to that problem was an internal-medicine clinical scribe paid hourly, or an offshore transcription service with a turnaround time longer than the patient's next visit. As of May 20, 2026, the answer is a 7B-class specialized model that demonstrably beats a frontier generalist on medical-terminology accuracy — and the buying decision that follows changes the Fort Wayne healthcare AI procurement stack at a layer most practices have not yet evaluated.
VentureBeat reported on May 20 that Corti's Symphony speech-to-text model — a vertical model trained on clinical conversation — beats OpenAI's general-purpose speech-to-text on medical-terminology accuracy. The release is the cleanest piece of specialized-vs-generalist evidence the AI market has produced this quarter. For Allen County urgent-care clinics, DeKalb County independent primary-care practices, and the long tail of dental, specialty, and behavioral-health practices serving Fort Wayne and Northeast Indiana, the release lands on a buying-decision layer that earlier Cloud Radix writeups deliberately did not cover. The Fort Wayne healthcare AI vetting playbook covered evidence vetting — whether to trust a vendor's claim. The Fort Wayne OpenAI privacy filter playbook covered PHI scrubbing — what to do with protected health information once it has been captured. Specialized-vs-generalist is the upstream question both writeups assumed: before you vet a vendor's claim, before you scrub PHI, you decide whether the model class is right for the task in the first place.
Key Takeaways
- Specialized clinical AI models now demonstrably outperform frontier generalist models on domain-critical metrics like medical-terminology accuracy — the architectural default for clinical documentation has shifted.
- The specialized-vs-generalist decision is modular, not all-or-nothing. The right pattern is specialized models at the input boundary (clinical STT, clinical entity extraction) and generalist models behind the Secure AI Gateway for downstream tasks.
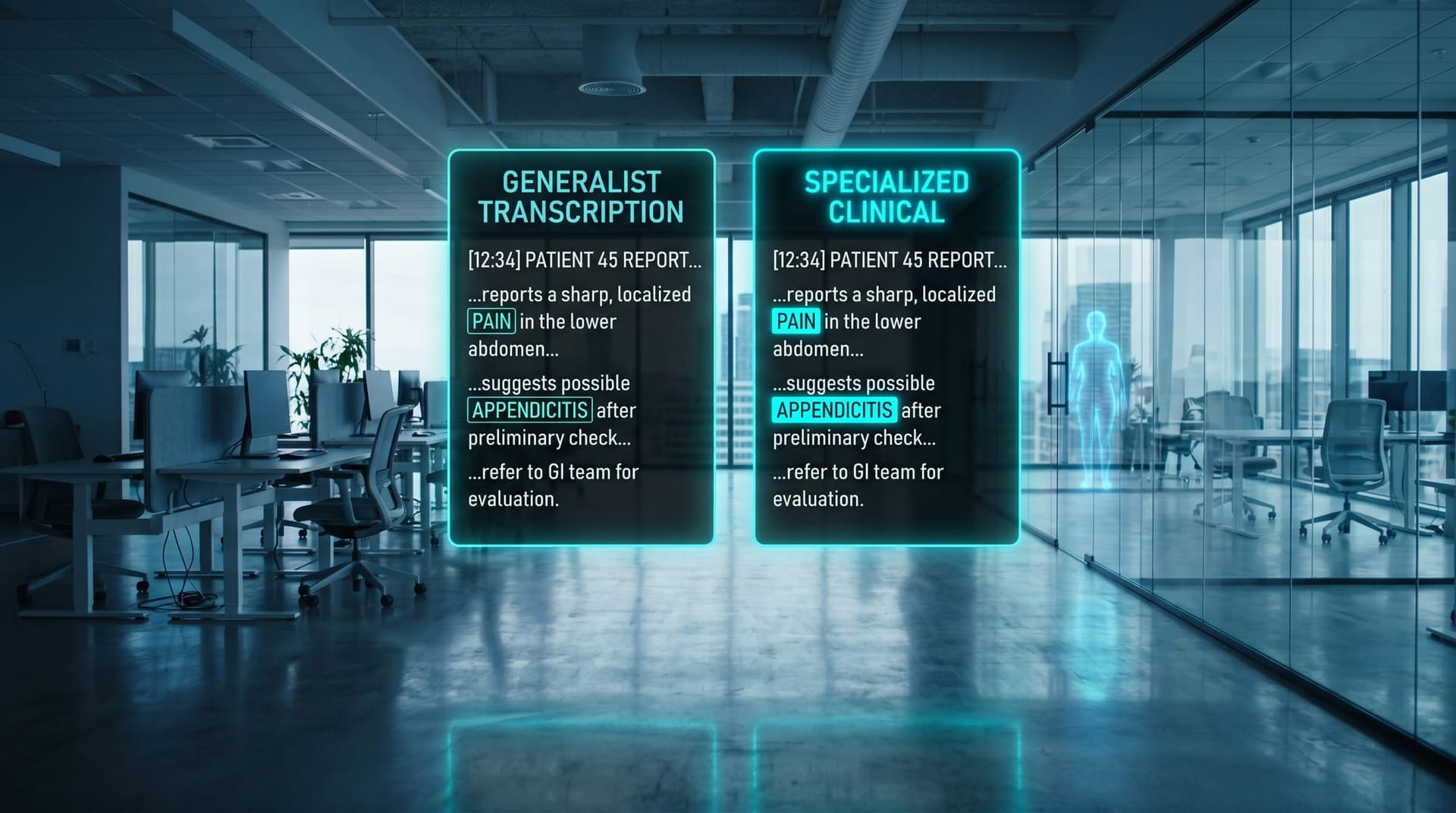
- Same-prefix clinical errors like “metformin” versus “metoprolol” are the failure mode that matters: generalist transcription produces them at a rate that becomes a liability event waiting for the right plaintiff.
- HIPAA posture is the gating filter. A specialized model that requires sending PHI to a vendor SaaS is a non-starter for most NE Indiana practices unless the entire pipeline operates under a Business Associate Agreement.
- The 4-question Specialized-vs-Generalist Buyer Test runs in a single afternoon and produces a defensible procurement decision for each task layer in your clinical AI Employee stack.
- Cloud Radix's recommended NE Indiana clinical AI Employee architecture: specialized clinical STT at input, generalist LLM behind the Secure AI Gateway for SOAP-note generation, generalist workflow agent for EHR filing, and a buyer-owned audit trail across all three layers.
Why is the generalist-AI default wrong for clinical documentation?
The mid-market AI Employee default — the architectural assumption Cloud Radix has documented across most of 2026 — is that a single frontier generalist model (Claude Sonnet, GPT-5.5, Gemini 3.5) covers nearly every AI Employee task, with vertical specialized models reserved for unusual edge cases. That assumption is structurally correct for most professional-services and operations workloads. It is structurally wrong for clinical documentation, and the Corti Symphony release is the first widely-circulated proof point.
The reason is the shape of the error distribution. Generalist speech-to-text models are trained on broadly distributed audio data — podcasts, audiobooks, conversation, meetings — and are optimized for general-purpose word-error rate. They handle the medical-terminology long tail by approximation: when the audio is ambiguous and the prior probability of any specific term is low, the model emits whichever phonetically plausible candidate is most common in its training distribution. For a clinician dictating “metformin 500 milligrams” with a slight enunciation variation, the model's prior is influenced by every non-clinical use of similar-sounding words in its training set. The result is a class of errors that a generalist model produces at a non-trivial rate and a specialized clinical model produces at a near-zero rate.
The error class matters because the errors are clinically indistinguishable from correct transcriptions to a non-clinician reviewer. A SOAP note that reads “metformin 500mg” instead of “metoprolol 500mg” is not a typo a billing clerk catches; it is a documented prescription discrepancy that surfaces, at the worst possible time, when a patient interaction goes wrong and the chart is pulled. The dexamethasone-versus-desmopressin pair, the cefazolin-versus-cefepime pair, the morphine-versus-hydromorphone pair — all are same-prefix or same-syllable substitutions that a generalist transcription produces and a specialized clinical transcription does not. The HHS HIPAA Security Rule treats the integrity of electronic protected health information as a baseline obligation, and a model class that systematically introduces clinically-material errors into the documentation is, in our reading, an integrity issue under that rule.
The structural conclusion is not that generalist models are dangerous everywhere in clinical work. It is that they are dangerous at the input boundary of clinical documentation — the boundary where audio becomes text — and that the architectural default for that boundary has shifted as of the Corti release.
What is the same-prefix clinical failure mode?
A worked example clarifies the stakes. Consider a Fort Wayne primary-care physician dictating into a generalist transcription product during a routine visit. The dictation includes the phrase “patient continues on metformin five hundred milligrams twice daily.” The model receives an audio signal whose acoustic features for “metformin” and “metoprolol” are similar enough that, absent a strong clinical prior, the generative posterior over candidate words is genuinely uncertain.
Metformin is a first-line oral diabetes medication. Metoprolol is a beta-blocker for hypertension and heart-failure management. Both are common in primary-care practice. Both are five-syllable words starting with “met-.” The dosage range overlaps — metformin is commonly prescribed at 500mg or 1000mg, metoprolol at 50mg or 100mg, with the 500mg figure plausible for metformin and implausible for metoprolol but not so implausible that a generalist model with no clinical prior would flag it.
A generalist model emits the higher-probability candidate from its general training distribution. A specialized clinical model emits the higher-probability candidate conditional on the clinical-document context, the patient's known prescription history if available, and the medication-name distribution observed in clinical training data. The difference is not a theoretical accuracy gain on a benchmark; it is the difference between a clinically correct SOAP note and a documented prescription discrepancy.
The same dynamic applies to dexamethasone (a corticosteroid) versus desmopressin (an antidiuretic hormone analog), cefazolin (a first-generation cephalosporin antibiotic) versus cefepime (a fourth-generation cephalosporin with a different spectrum and contraindication profile), and many other clinically distinct pairs that share acoustic features. The ONC SAFER Guides — the Office of the National Coordinator's safety reference for health-IT systems — explicitly call out medication-list accuracy as a class of error that can propagate through downstream clinical decision support and produce patient harm. A model class that systematically increases the probability of these errors at the documentation layer is a procurement risk a NE Indiana practice owner can no longer wave away as “we will catch it on review.”
What is the specialized-vs-generalist architectural pattern Cloud Radix recommends?
Specialized-vs-generalist is not all-or-nothing. The right pattern is modular: specialized models at the input boundary where domain-critical accuracy is decisive, and generalist models behind the Secure AI Gateway for downstream tasks where general reasoning, summarization, and workflow execution are the load-bearing capabilities. The Gateway is the modular boundary that lets a clinical AI Employee program mix specialized and generalist components without locking the whole stack to one vendor.
Concretely, a Fort Wayne clinical AI Employee program runs as follows. Specialized clinical STT transcribes the encounter audio inside the customer's environment or behind a Business-Associate-Agreement-covered vendor endpoint, producing a verbatim transcript with clinical-terminology accuracy that the generalist class cannot match. Specialized clinical entity extraction — also a vertical model class — runs against the transcript to identify medications, dosages, problems, procedures, and ICD-10-coded findings. The transcript and the extracted entities then pass through the Secure AI Gateway, where PHI redaction, audit logging, and access-control policy decisions happen at the customer's boundary rather than at any vendor's discretion. Generalist LLM tasks — SOAP note structure generation, patient-friendly summary, billing-code suggestion narrative — run downstream of the Gateway against the redacted, structured representation; these tasks are reasoning-heavy and benefit from frontier generalist capabilities. Generalist workflow agents — the components that file the completed note to the EHR, route the prescription to the pharmacy, schedule the follow-up — run in a separate orchestration layer and are again generalist territory.
The architectural payoff is procurement flexibility. The buyer can swap the specialized clinical STT vendor without touching the generalist LLM behind the Gateway. The buyer can swap the generalist LLM without touching the specialized clinical STT. The vendor that wants to sell the whole stack — and most do — is offered the same boundary contract as any other vendor: you connect to the customer's Gateway, you operate under the customer's BAA, you submit to the customer's audit cadence, you do not see the customer's PHI in cleartext outside the agreed-upon scope. The buyer-owned Fort Wayne AI vendor release-pipeline buyer test applies to specialized clinical vendors as much as to generalist ones; Corti is now one of the candidates to score against that test.

What is the HIPAA posture trade-off for specialized clinical models?
The HIPAA posture filter is where most specialized-vs-generalist procurement decisions actually break. A specialized model that produces excellent transcription accuracy but requires sending raw PHI to a vendor SaaS is, for most NE Indiana practices, a non-starter. The HIPAA Privacy Rule and Security Rule together require a Business Associate Agreement with any third party that processes PHI on the covered entity's behalf, and the practical reality for a 4-to-15-provider practice is that negotiating, auditing, and maintaining BAAs with multiple model vendors is a heavier compliance lift than most administrators have capacity for.
The deployment options for a specialized clinical STT model are, in order of compliance burden: a self-hosted deployment inside the customer's environment (no BAA needed because no third party touches PHI); a vendor-hosted deployment under a BAA with a vendor whose security posture has been independently audited (BAA needed, audit cadence needed); a vendor-hosted deployment without a BAA (effectively non-compliant for PHI workloads). The third option is unfortunately how many specialized AI vendors initially market their products to small healthcare practices; the Fort Wayne air-gapped AI sovereign Gemini writeup covered the sovereign deployment pattern that addresses the most stringent posture requirements.
The Gateway-side architecture covered above is HIPAA-friendly by construction. PHI never leaves the customer's boundary in cleartext; the specialized model either runs inside the customer's environment or under a BAA-covered endpoint; the audit trail of who read what is generated at the customer's Gateway rather than at the vendor's discretion. The Indiana Code Title 16 state-level patient privacy provisions sit on top of HIPAA and do not change the architectural recommendation, but they raise the procurement-due-diligence requirement for any out-of-state vendor whose data-residency posture is unclear.
The compounding posture — specialized models at the input boundary plus air-gapped deployment for the entire pipeline — is achievable and is the recommended baseline for Fort Wayne and Northeast Indiana practices handling high-acuity or behavioral-health work. For lower-acuity primary-care, dental, and specialty work, the BAA-covered vendor-hosted specialized model behind the Gateway is the more common and operationally sustainable pattern.
What is the Specialized-vs-Generalist NE Indiana Healthcare Task Matrix?
The matrix below is the body's spine. Read it as the one-page version of the architectural recommendation. Each row is a clinical AI Employee task layer; the columns are the decision dimensions a Fort Wayne practice owner needs to evaluate.
| Task layer | Specialized model exists | Generalist sufficient | HIPAA posture | Cloud Radix recommendation |
|---|---|---|---|---|
| Clinical STT (encounter transcription) | Yes — Corti Symphony and others | No — same-prefix medication errors are clinically material | Self-hosted or BAA-covered endpoint required | Specialized at input boundary |
| Clinical entity extraction (medication, problem, procedure, ICD-10) | Yes — clinical NLP vendors | Partial — frontier generalists handle named entities but miss clinical nuance | Same as STT layer | Specialized at input boundary |
| SOAP note structure generation (from transcript + entities) | Limited — most vendors compose generalists with clinical prompts | Yes — frontier generalist behind Gateway is the workhorse | Gateway-side: PHI is redacted into structured tokens before LLM call | Generalist behind Secure AI Gateway |
| EHR filing and workflow automation | Limited — EHR-specific integrations exist | Yes — generalist workflow agents handle integration patterns | Audit trail required for every write to the EHR | Generalist behind Secure AI Gateway |
| Patient-facing chat (appointment, instructions, follow-up) | Limited — clinical chat vendors exist for triage | Yes for non-triage, with PHI controls | BAA required for any PHI exposure | Generalist behind Secure AI Gateway with explicit triage exclusion |
The pattern is consistent: specialized models earn their place at the input boundary of the pipeline, where domain-critical accuracy is decisive. Behind the Gateway, where reasoning, summarization, and workflow are the load-bearing capabilities, generalist models are the right default. This is structurally similar to the principle covered in the Fort Wayne Microsoft Copilot prompt injection risk writeup: a generalist model is not categorically wrong in a regulated environment, but the boundary it operates within must be explicitly architected.
What does this look like for three NE Indiana clinical scenarios?
The architectural pattern lands differently across the three most common NE Indiana clinical procurement situations.
An Allen County urgent-care clinic processing 60 to 120 encounters per day across three to five providers should adopt specialized clinical STT at the encounter-transcription layer, with the model either self-hosted on clinic infrastructure (preferred) or hosted by a BAA-covered vendor with an independent SOC 2 Type II attestation. The downstream SOAP-note generation runs against a generalist LLM behind the Gateway; the redacted transcript and the extracted clinical entities are the inputs, the structured SOAP note is the output, and the clinician reviews and signs before the note enters the EHR. The total architecture supports the volume without adding latency to the clinical workflow.
An Allen County dental practice running a four-chair operation with a strong patient-communication workload should adopt specialized clinical STT only if the dental workflow includes regular dictation — many smaller dental practices do not, and the generalist transcription class may be acceptable for the documentation patterns dental work actually produces (chart notes are often shorter and more codified than primary-care SOAP notes). The patient-facing chat and recall-scheduling AI Employee components run generalist behind the Gateway, with explicit exclusion of clinical-triage use cases. The Fort Wayne AI phone agents writeup covered the multi-vendor voice stack pattern that often shows up in dental practice phone-handling; the specialized-versus-generalist question applies at the customer-service layer too, though the answer is usually generalist with structured prompts rather than specialized.
A DeKalb County independent primary-care practice running two to four providers should adopt the same architecture as the urgent-care scenario but at a smaller scale. The BAA-covered vendor-hosted specialized STT is typically the right deployment choice — the practice rarely has the in-house infrastructure to self-host — and the Gateway-side generalist for SOAP-note generation is the workhorse. The EHR-filing workflow agent generalist completes the loop. Total architectural footprint: one specialized vendor for STT, one generalist vendor for LLM, one Secure AI Gateway operated by Cloud Radix, one set of audit logs in the practice's storage.
The common thread across all three is the modular boundary at the Gateway: specialized models at the input, generalist models behind the Gateway, buyer-owned audit trail across both.

What is the Specialized-vs-Generalist Buyer Test for NE Indiana healthcare?
The test below is four questions, each answerable in under thirty minutes per task layer, with an acceptable-answer band. Run it across each of the five task layers in the matrix above. The output is a defensible procurement decision per layer.
1. Does the task involve clinical vocabulary with same-prefix-different-meaning failure modes?
Examples: metformin versus metoprolol, dexamethasone versus desmopressin, cefazolin versus cefepime, morphine versus hydromorphone. If the task layer regularly produces or processes content where these substitutions are clinically material, specialized is the right model class. If the task layer is downstream of structured representations (medication codes, ICD-10 codes, structured intake forms), generalist is typically sufficient.
2. Does the specialized model publish a head-to-head WER or accuracy delta against a frontier generalist?
A specialized vendor that cannot show a head-to-head benchmark against a frontier generalist — Whisper, the OpenAI STT model, the Google Cloud Speech-to-Text medical variant, the Microsoft Azure equivalent — has not earned the specialized-model premium. A specialized vendor that publishes a delta of more than two percentage points on medical terminology, replicable on the buyer's own audio sample, has. The vendor-claim vetting layer covered earlier is the broader frame; this question is the specialized-model-specific instance of that vetting.
3. Is the specialized model deployable behind the Secure AI Gateway without sending PHI to a vendor SaaS?
The acceptable deployment options are self-hosted on customer infrastructure, BAA-covered vendor endpoint with an independent security attestation, or hybrid (specialized inference inside the Gateway with vendor-supplied model weights). The non-acceptable option is “send the audio to our cloud” without a BAA and without an audit-cadence commitment. The sovereign-deployment pattern covered earlier is the most stringent posture available, and specialized clinical models are usually deployable in that pattern.
4. Does the architecture preserve modular swappability across task layers?
The acceptable architecture is one where the specialized STT vendor can be replaced without changing the generalist LLM behind the Gateway, and vice versa. The non-acceptable architecture is the all-in-one vendor lock — a vendor that bundles STT, entity extraction, SOAP generation, and EHR filing and refuses to expose the intermediate representations the modular pattern depends on. The modular boundary at the Gateway is the load-bearing architectural commitment; vendors that resist it should be deprioritized.
The four-question test produces a per-layer recommendation. Run it across the five layers in the matrix and the output is a complete clinical AI Employee procurement plan, with explicit specialized-vs-generalist calls at each layer and explicit HIPAA posture commitments at each vendor.

How does Cloud Radix run a 6-week clinical AI Employee pilot for Fort Wayne practices?
Cloud Radix runs a six-week clinical AI Employee pilot for NE Indiana healthcare practices in the 4-to-15-provider range. Week 1 is the channel-and-task inventory and the specialized-vs-generalist buyer test across the five task layers. Weeks 2-3 stand up the specialized clinical STT integration — either self-hosted on practice infrastructure or BAA-covered vendor endpoint — and the Secure AI Gateway boundary that PHI redaction and audit logging run through. Week 4 integrates the generalist LLM for SOAP-note generation against the redacted transcripts. Weeks 5-6 integrate the EHR-filing workflow agent and complete the end-to-end pipeline against a clinician-supervised pilot caseload.
The pilot deliverable is a working clinical AI Employee against one clinical workflow (encounter transcription, SOAP note, EHR filing), a written architecture document, a BAA file covering every vendor in the pipeline, an audit-log baseline, and a written change-management plan for expansion from the pilot to production. The pilot is sized to fit a practice with no full-time IT staff; Cloud Radix runs the architecture work and the practice owns the operational policy and the clinical-review cadence after the pilot. Cloud Radix's AI Employees service for healthcare ships behind the Secure AI Gateway by default and supports the modular specialized-plus-generalist pattern this post describes.
The honest framing is that the specialized-vs-generalist decision is more important than which specific specialized vendor you pick. Corti Symphony is the freshest evidence point as of May 20, 2026, but the architectural commitment — specialized at input, generalist behind the Gateway, buyer-owned audit trail — outlives any single vendor's product roadmap. The NIST AI Risk Management Framework's Govern function and the OWASP Top 10 for LLM Applications 2025 jointly recommend the kind of modular boundary architecture this post describes, and the recommendation does not change when a new specialized vendor ships next quarter.
Frequently Asked Questions
Q1.What does "specialized AI" mean in a clinical documentation context?
Specialized AI in this context means a model class — typically smaller in parameter count than a frontier generalist — trained on domain-specific data (clinical conversation, clinical text, medical terminology) and optimized for domain-critical metrics rather than general-purpose ones. Corti Symphony is a specialized clinical speech-to-text model. Specialized clinical entity extraction, specialized clinical vision (for image triage), and specialized clinical question-answering are sibling categories. The specialized model trades off general-purpose capability for domain accuracy, and on domain-critical tasks the trade is increasingly favorable.
Q2.Should a Fort Wayne primary-care practice replace its current dictation product with a specialized clinical model?
Likely yes at the encounter-transcription layer, after running the specialized-vs-generalist buyer test against the current vendor's published accuracy data. The replacement is not a wholesale rip-out — the existing EHR, billing, and workflow infrastructure stays in place; the change is at the audio-to-text layer specifically. The right cadence is a four-week side-by-side pilot in which the specialized model runs in parallel with the incumbent dictation product, both run against the same encounter audio, and the practice compares medical-terminology accuracy, clinician edit time, and total cost.
Q3.What is the HIPAA-compliant deployment pattern for a specialized clinical STT model?
The compliant deployment options are self-hosted on customer infrastructure (no third party touches PHI, no BAA needed at the model layer), or vendor-hosted under a Business Associate Agreement with an independent security attestation (SOC 2 Type II or equivalent). Vendor-hosted without a BAA is non-compliant for PHI workloads. The Secure AI Gateway sits in front of either deployment to handle PHI redaction, audit logging, and access-control policy at the customer's boundary.
Q4.How does specialized AI fit with the rest of the clinical AI Employee stack?
Specialized models earn their place at the input boundary — clinical STT and clinical entity extraction, primarily. Behind the Secure AI Gateway, the downstream tasks (SOAP-note structure generation, EHR filing, patient-facing chat) run against frontier generalist models because reasoning, summarization, and workflow execution are the load-bearing capabilities there. The Gateway is the modular boundary that lets specialized and generalist components compose without locking the whole stack to one vendor.
Q5.What happens if a vendor only sells the whole stack and refuses the modular architecture?
Deprioritize that vendor. A vendor that bundles STT, entity extraction, SOAP generation, EHR filing, and patient-facing chat into a single proprietary stack and refuses to expose the intermediate representations is offering vendor lock-in, not architecture. The procurement risk of the all-in-one stack — switching cost, BAA portability, audit-trail control, end-state cost growth — is higher than the operational savings the bundle offers. Cloud Radix's recommended posture is to favor vendors that respect the Gateway-side modular boundary.
Q6.Is Corti Symphony the only specialized clinical AI model worth evaluating?
No, but it is the freshest evidence point as of May 20, 2026, and the head-to-head accuracy claim against OpenAI on medical terminology is the strongest publicly-documented case for the specialized model class on this task. Other specialized clinical AI vendors include the existing clinical NLP and clinical STT incumbents; the Specialized-vs-Generalist Buyer Test in this post applies equally to all of them. Cloud Radix's pilot framing is designed to keep the specialized-vendor choice swappable.
Q7.How should a small NE Indiana practice budget for a clinical AI Employee program with specialized models?
The typical cost structure has three lines: the specialized model layer (per-minute or per-encounter pricing, depending on vendor), the generalist LLM layer behind the Gateway (per-million-token pricing), and the Secure AI Gateway plus Cloud Radix architectural support (a flat operational fee). For a 4-to-15-provider practice, the combined annual operating cost is typically in the low-to-mid five figures, with the specialized model layer the dominant line. The pilot is sized so the practice can validate the cost projection against actual usage before committing to a production rollout.
Sources & Further Reading
- VentureBeat: venturebeat.com — Corti's new Symphony for Speech-to-Text model beats OpenAI at medical terminology accuracy — the specialized-vs-generalist evidence point that anchors this post.
- U.S. Department of Health and Human Services: hhs.gov — HIPAA Security Rule — integrity-of-PHI obligations that map onto clinical-AI transcription accuracy.
- U.S. Department of Health and Human Services: hhs.gov — HIPAA Privacy Rule — Business Associate Agreement baseline for vendor-hosted PHI processing.
- U.S. Office of the National Coordinator for Health IT: healthit.gov — SAFER Guides — medication-list accuracy as a class of error with downstream clinical impact.
- NIST: nist.gov/itl/ai-risk-management-framework — AI Risk Management Framework Govern function recommending modular boundary architecture.
- OWASP GenAI Security Project: genai.owasp.org/llm-top-10/ — OWASP Top 10 for LLM Applications 2025 referenced for the data-handling baseline.
- Indiana General Assembly: iga.in.gov — Indiana Code Title 16 — state-level health and patient-privacy provisions layered on top of HIPAA.
Run a Clinical AI Employee Pilot for Your Practice
We map the specialized-vs-generalist decision against your clinical workflows, deploy a 6-week pilot behind a Secure AI Gateway, and ship a buyer-owned audit trail across every layer — sized to fit a Fort Wayne practice with no full-time IT staff.